

PCOS. You may have heard this term from a friend, read an article about it, or have absolutely no idea what it means. It’s important to bring awareness to PCOS because it effects 1 in 10 women of childbearing age.
PCOS stands for Polycystic Ovarian Syndrome and it is a complex hormonal and metabolic condition.
Despite the name, it is not always characterized by cysts on the ovaries.
Other symptoms of PCOS include acne, irregular menstrual cycles (<10 per year of cycles >35 days), androgenic alopecia (hair loss, usually starting where hair is parted), hirsutism (dark body hair growth), visceral fat, acanthosis nigricans (dark discoloration in the folds of skin), weight gain or difficulty losing weight, and skin tags.
In order to be diagnosed with PCOS, a woman has to have two of the following criteria:
- Irregular or no ovulation
- Hyperandrogenism (elevated male sex hormones) as characterized by lab testing or symptoms
- Polycystic ovaries as seen on a transvaginal ultrasound (≥12 follicles per ovary)
PCOS can NOT be diagnosed based on Anti-Müllerian, follicle stimulating, or luteinizing hormone levels. It also can’t be diagnosed based on weight or BMI, insulin levels, or hemoglobin A1c.
Hyperandrogenism means elevated levels of androgens in females. This is what can cause androgenic alopecia, acne, and hirsutism. When a woman goes in for a transvaginal ultrasound, they are typically looking for the “string of pearls.” This is the ultrasound sign of multiple small (<5mm) follicles peripherally located on the ovaries and is thought to represent abnormal accumulation of immature follicles, a characteristic of PCOS.
There are four different types of PCOS, so women may carry their diagnosis different, with different symptoms.
- Type A: High androgens/androgenic signs, irregular periods or delayed ovulation, polycystic ovaries
- Type B: High androgens/androgenic symptoms, irregular periods or delayed ovulation, normal ovaries
- Type C: High androgens/androgenic signs, regular periods (<35 days), polycystic ovaries
- Type D: Normal androgens, irregular periods or delayed ovulation, and polycystic ovaries
There are several metabolic health risks associated with PCOS including:
- Type 2 diabetes, with >50% of women with PCOS diagnosed by age 40
- Gestational diabetes
- Heart disease, with 4-7x higher risk for heart attack
- Dyslipidemia (with elevated LDL cholesterol levels and decreased HDL cholesterol levels)
- Infertility
- Hypertension
- Obesity, effecting 30-70% of women
- Metabolic syndrome, effecting 1/3 of women
- Eating disorders
- Cancers, with 3x increased risk for endometrial cancer
- Sleep apnea and other sleep disorders
- Other hormone related conditions, like hypothyroidism.
PCOS is often accompanied by insulin resistance, effecting 75% of lean and 95% of overweight women. First, what is insulin resistance? Insulin is a hormone secreted by the pancreas to help carry glucose into your cells. With insulin resistance, your cells don’t respond normally to insulin and glucose can’t enter the cells, causing a build up of glucose in the blood.
Why does this happen in conjunction with PCOS though?
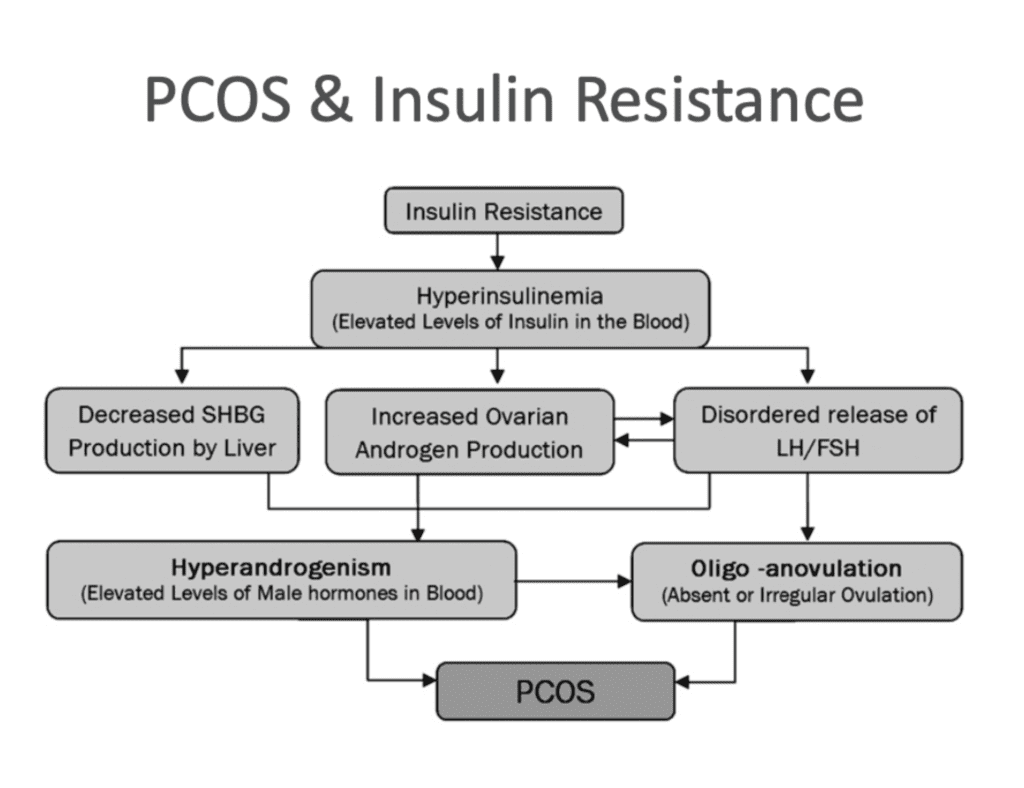
The increased insulin levels tell the ovaries to increase androgen production, namely testosterone, which leads to decreased production of sex-hormone binding globulin (which transports testosterone through the blood in its inactive form) and therefore, elevated levels of testosterone. Excess levels of androgens are associated with increased abdominal fat gain, which can make inflammation and insulin resistance worse, and then the cycle just continues. Furthermore, the ovarian tissues of women with PCOS have been shown to be hyper-responsive to insulin, which is why high levels of excess testosterone are produced.
This cycle is also the cause of absent or irregular ovulation. The graph at the end of this article gives an example of the mechanisms taking place.
How is PCOS medically treated?
Traditional methods of treatment for PCOS include hormonal birth control, anti-androgen medications, fertility medications, anti-obesity medications, insulin-sensitizing medications (metformin), diet, lifestyle, and supplements.
Why does diet and lifestyle matter?
Diet and lifestyle management are great contributors to overall health status, but they are especially important for women with PCOS or other hormonal conditions. There is no “one size fits all” when it comes to dietary and lifestyle modifications. Numerous factors need to be taken into consideration such as: food preferences, cultures, accessibility, lifestyle, activity level, concurrent medical issues, and overall goals.
Over the years, there have been many suggestions that carbohydrates are the enemy of those with PCOS because of insulin resistance. Many choose to eliminate carbs, causing fear and unhealthy relationships with food. It is also common to hear that those with PCOS should eat very little, having much slower metabolisms than women without PCOS. This can lead to inadequate food intake for overall health, causing the metabolic symptoms of this condition to become even worse. This may lead to women feeling like they are a failure and throwing in the towel when it comes to focusing on their health and alleviating symptoms. This can also lead to the development of eating disorders, particularly Binge Eating Disorder due to restriction of food or macronutrients.
Numerous studies have been done to try to figure out what the best diet for those with PCOS is. The conclusion? There is no one “ideal diet” for PCOS. Instead, the focus should be on overall intake and quality of the food consumed, especially when it comes to carbohydrates. A diet rich in high-fiber vegetables, fruits, legumes, and whole grains while limiting processed foods and added sugars is crucial for PCOS management.
Lifestyle factors should include exercise (but not HIIT, or at least not a lot of it), quality sleep, stress management, and environmental exposures.
Exercise:
There are numerous benefits of exercise for PCOS. Exercise increases insulin sensitivity and lowers glucose levels, lowers testosterone, burns calories, increases metabolism, increases lean body mass, and may improve ovulation, menstrual regularity, and pregnancy rates. Exercise can also improve lipid profile, aid in stress management, and improve your mood. Weight training is usually recommended for those with PCOS, due to better management of adrenal hormones associated with exercise.
Sleep:
Women with PCOS are at increased risk for insomnia, daytime sleepiness, and obstructive sleep apnea, regardless of their weight. <6 hours of sleep/night is linked to higher fasting insulin levels and an increased risk for insulin resistance. If you need to improve your sleep, a few tips to help would be to avoid electronics and stimulation before bed, sleeping in a cool, dark room, and drink herbal teas or have a warm bath before bed.
Stress:
Adrenal hormones can play a role in hyperandrogenism. Studies on the effects of stress management techniques in PCOS are limited BUT in other chronic conditions, such as Type 2 Diabetes, meditation, deep breathing, yoga, time in nature, and behavioral therapy have been shown to be effective.
Environment:
Endocrine disrupting chemicals have been proposed in the etiology of PCOS. In one study, adolescents with PCOS had increased BPA levels compared with their controls. Serum BPA levels have been found to correlate with serum testosterone levels. In another study, women with PCOS had higher levels of certain PFCs compared with controls.
Are there any supplements that help with PCOS?
First, all supplements should be individualized and account for diet, nutrient deficiencies, lifestyle, and concurrent medical issues.
One of the most promising supplements is Inositol. It has been researched in hundreds of studies in PCOS. When head-to-head with metformin, Inositol has been shown to be as effecting at improving insulin sensitivity and inducing ovulation.
Vitamin D deficiency is common in PCOS and low Vitamin D levels have been linked to insulin resistance. Levels should be evaluated by a primary care physician before taking any vitamin D supplements.
How does coaching contribute to PCOS management?
Due to there being several different types of PCOS, management requires a personalized approach, incorporating diet, lifestyle, and supplements. Having an educated coach on your side to help you find what approach works best for you can make a world of difference in the management of this condition.
Having a coach who understands the metabolic and hormonal processes at play can empower you with education so you can learn about this condition and not feel lost. Coaching also provides invaluable support and a sense of community, so you don’t have to go through this alone.
PCOS is one of the most misunderstood conditions that effects so many women. Throughout my coaching career, I have personally helped a few dozen women navigate their way through their diagnosis, treatment, and dietary and lifestyle modifications.
Your diagnosis isn’t the end of the road. There’s a way through it, and coaching can help guide you.
-Coach Dev
CEO
Arrow Nutrition and Training, LLC

